




Molly’s story: Human connection and innovative surgery helps teen with scoliosis
Molly’s story: Human connection and innovative surgery helps teen with scoliosis
55 Fruit Street
Yawkey Center for Outpatient Care, Suite 3E
Boston,
MA
02114
Anterior vertebral tethering (AVT), also known as vertebral body tethering (VBT) or, simply, tethering, is a treatment option for patients with severe, progressive scoliosis who are contemplating surgery, but wish to correct their scoliosis without sacrificing growth, motion or function of the spine. The surgery that is most often performed for progressive scoliosis is called a “posterior spinal fusion with instrumentation.” It is also known simply as a spinal arthrodesis or fusion. The goal of this surgery is to create a solid “fusion” of the curved part of the spine.
Spinal fusion is created by operating on the bones of the spine (vertebrae), manipulating and correcting some of the curve/rotation of the spine, adding bone graft, and allowing the vertebral bones and bone chips to slowly heal together to form a solid mass of bone. The hardware that is placed (rods, hooks, and screws) serves as an internal “cast” while the fusion is allowed to heal and become solid. The bone graft may come from your hip (autologous iliac crest bone graft) or more likely from the hospital’s bone bank (allograft). This spinal instrumentation is left in your back and should not cause any problems.
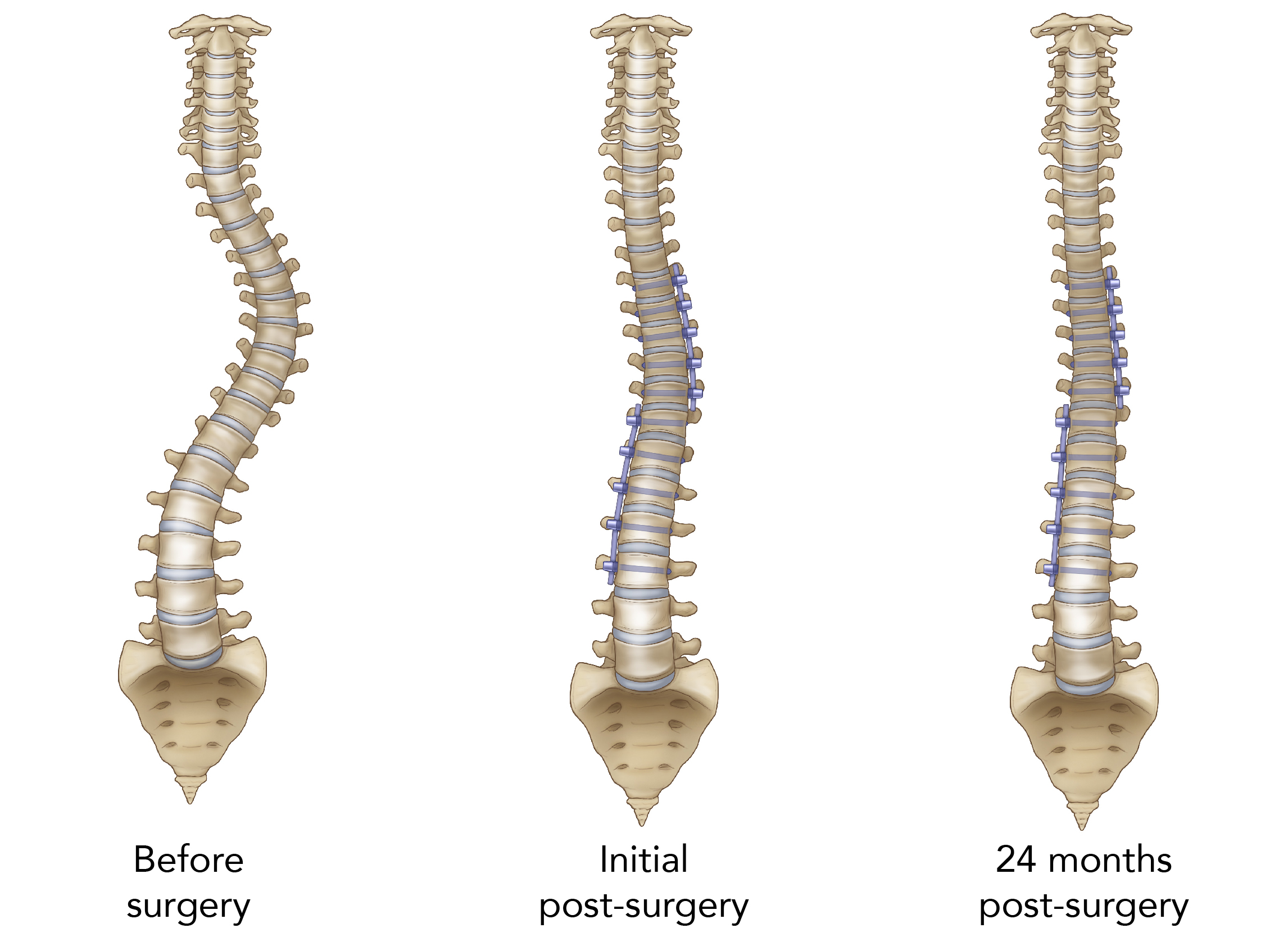
However, AVT is an alternative to spinal fusion surgery wherein a flexible cord or “tether” is implanted in the back for gradual scoliosis curve correction. AVT is more physiologic than fusion surgery and avoids the creation of a rigid bone graft in your back. This minimally invasive approach allows endoscopic treatment of thoracic curves and mini-open exposures for lumbar curves. And, in contrast to the two-step procedure required for fusion, AVT requires only the instrumentation step. AVT also requires less operative time, less blood loss and fewer implants, with no bone graft requirement for fusion. Post-operative recovery is faster, with decreased length of hospital stay and a more rapid return to a higher level of function. Experts believe that scoliosis correction with AVT may also be safer neurologically, not only due to the flexibility of the correction, but also because correction occurs gradually over time.
Due to advances in surgical technology, Mass General surgeons implant the tether along the spine by making three small (2.5 cm) incisions, or portals, in a line beneath the armpit. Working endoscopically (through a tube inserted in the portal), an anchor and bone screw are placed into the patient's spine on the side of the spinal curvature. The tether cord is secured to the bone screws using set screws. During surgery, the surgeon will apply tension to the tether cord to partially straighten the patient's spine. After surgery, the tether cord continues to straighten the spine while the patient grows. The duration of AVT surgery depends on the severity of the spinal curvature being addressed and the length of the tether being implanted. AVT surgeries typically last two to three hours for single curvatures and four to six hours for double curvatures, with an average hospital stay of three nights. Many patients are upright and walking within a day or two of their surgery.
As the patient recovers, they lie on their back in the recovery room or post-anesthesia care unit (PACU). They may feel stiff from being in one position for a long time. Usually, patients will remain in the recovery room for two to three hours while they recover from the surgery and anesthesia. It is possible to have a parent visit in the PACU after they have met with the spine surgeon. The PACU is located on White 3 next to the Main OR.
Patients most likely will spend one night in the Pediatric Intensive Care Unit (PICU) after AVT surgery. In the PICU, they will be monitored very closely. The PICU is in the Gray Bigelow building on the 6th floor. Parents will be able to visit and can stay in a nearby room on the floor (pending availability and current COVID restrictions). Patients will usually only spend one day in the PICU before moving to the adolescent floor (Ellison 18).
The adolescent floor is in the Ellison building on the 18th floor. Parents are welcome and encouraged to spend the night with their child. Child Life Specialists are dedicated to making the hospitalization as positive as possible. They help you in coping with illness/surgery, hospitalization, as well as separation from home, routine and friends. A new pediatric/adolescent playroom has recently been added to the floor. Television, video games, movies and other activities are also available.
It is common to feel quite tired following spinal surgery, and the patient may need help turning from side to side initially. They will meet with a physical therapist usually on the second post-operative day. The physical therapist will assist with deep breathing, coughing, mobility and endurance. Once given the okay by the surgeon, the patient may get out of bed and sit in a chair. The physical therapist will teach the patient the correct way to get out of bed and walk without twisting their spine, and will help them progress to walking short distances on the floor.
Individual pace of recovery is different for each patient and depends on the type and extent of surgery. The patient will be given additional information about specific activity restrictions at a follow-up visit, but AVT patients have been able to resume sports and exercise three months after surgery. Consult with your care team for a recovery plan tailored to your particular situation and needs.
Read more about preparing for spinal surgery
Read more about vertebral tethering at Mass General for Children
Children’s Orthopaedics at Mass General takes a coordinated team approach to scoliosis treatment. Three of our surgeons specialize in anterior vertebral tethering, and they work alongside a team of other orthopedic doctors, advanced practitioners and fellows who deliver high-quality, compassionate care to every adolescent who walks through our doors.
Have questions about anterior vertebral tethering? Get in touch.